

NIV
ONeal Medical currently carries:
LUISA
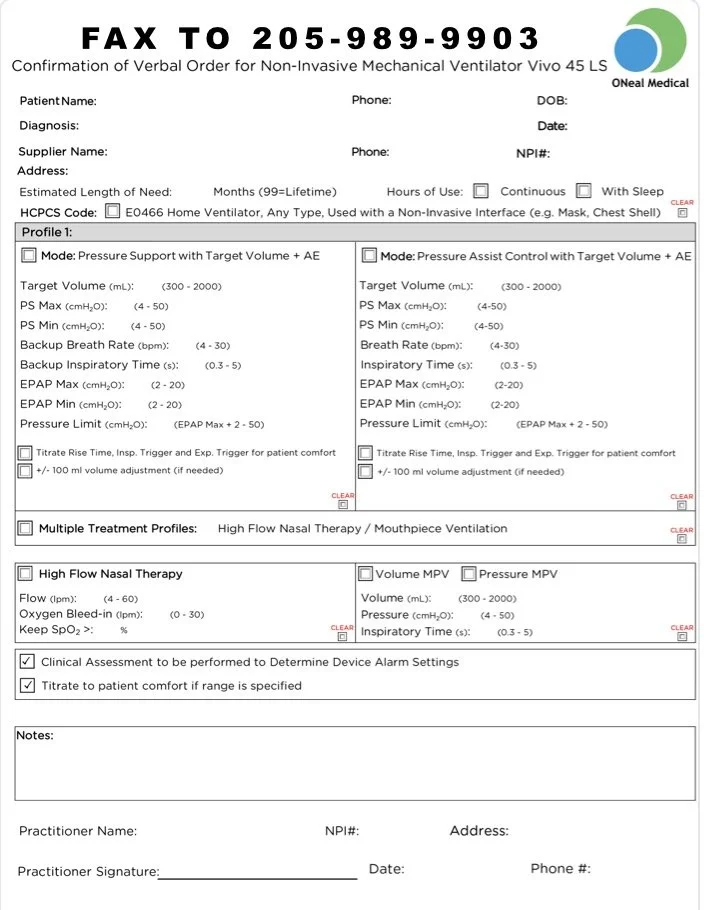
Vivo 45LS
We accept any prescription from for any of these ventilators and can make the proper clinical conversion of settings to accommodate the LUISA or 45LS.
IF the physician is brand specific for a vent, we will try and accommodate that request on a referral by referral basis.

NIV forms and handouts












NIV
Suggested Medical Necessity Statements for Prior Authorizations
copy/paste as needed or download the PDFs
-
A. Fast Appeal
Name:
Address:
DOB:
Member ID:
To Whom It May Concern,
I am requesting a fast appeal on the above patient ______________________. Due to the severity of the patient’s disease, bi-level pap devices have been proven ineffective at managing this patient’s hypercapnia. This patient requires a mode of non-invasive ventilation similar to AVAPS-AE to achieve adequate ventilation. Interruption or failure to provide NIV would quickly lead to exacerbation of the patient’s condition, hospital admission, and likely harm or death to the patient. The patient requires frequent durations of respiratory support and deteriorates quickly in the absence of non-invasive ventilation.
Ordering Physician:_________________________
NPI #: _______________________________
Date: _____________________
-
B. Expedited Pre-Auth
Name:
DOB:
Member ID:
Date:
To Whom It May Concern,
I am requesting an expedited pre-authorization for my patient _______________________. Non invasive ventilation similar to AVAPS-AE is a life sustaining mode and is medically necessary to prevent chronic respiratory failure. Interruption of respiratory support could quickly lead to serious harm and or death.
Ordering Physician: ________________________Physician Signature: ________________________
NPI #: _______________________________
Date: ____________________________
-
C. Letter of Medical Necessity
Name:
DOB:
Date:
Member ID:
To Whom It May Concern,
This letter serves as a letter of medical necessity for non-invasive ventilation with modes similar to AVAPS-AE. ______________________, is treated for chronic respiratory failure secondary to chronic obstructive pulmonary disease. BIPAP has been tried and failed and has proven the patient requires an NIV mode like AVAPS-AE to achieve adequate ventilation. The patient requires volume ventilation due to the severity of this patient’s disease state and life-threatening condition like carbon dioxide retention. Due to the increased probability of exacerbation, the patient requires a controlled target ventilation via face mask to prevent hospital admissions and death. The NIV will be used every night during sleep as well as on an as needed basic for naps and increased shortness of breath.
In my professional opinion, utilization of non-invasive ventilation in this patient will improve outcomes and reduce emergency room visits and hospital admissions in the future.
Sincerely,
Ordering Physician: ________________________
Physician Signature: _______________________
NPI#: __________________________________
Date: ___________________________
-
D. Letter of Medical Necessity
Name:
DOB:
Date:
Member ID:
To Whom It May Concern,
Home NIV ordered due to COPD and chronic respiratory failure. BIPAP/ BIPAP ST are deemed inappropriate therapies for the patient due to providing target tidal volumes via breath-by-breath auto-adjusting pressures. Home NIV does provide these patient specific settings and will deliver pressures within precise parameters that the COPD progression demands. The therapy will not only reduce the chronic Co2 retention (even while wearing BIPAP) but it will also allow the patient to remain stable in the home and out of the inpatient setting. We will educate on the usage and benefits of the NIV ventilator through our dedicated respiratory therapist and compliance will be reported back to my office.
Ordering Physician: ________________________
Physician Signature: __________________________
NPI: _______________________________
Date: ______________________________
E0482 “Cough Assist” devices
Philips T70, BiWave Cough, etc.
E0482 - Cough stimulating device, alternating positive and negative airway pressureA7020 INTERFACE FOR COUGH STIMULATING DEVICE, INCLUDES ALL COMPONENTS, REPLACEMENT ONLYB91 Sequelae of poliomyelitisE74.02 Pompe diseaseE74.05 Lysosome-associated membrane protein 2 [LAMP2] deficiencyG12.0 Infantile spinal muscular atrophy, type I [Werdnig-Hoffman]G12.1 Other inherited spinal muscular atrophyG12.20 Motor neuron disease, unspecifiedG12.21 Amyotrophic lateral sclerosisG12.22 Progressive bulbar palsyG12.23 Primary lateral sclerosisG12.24 Familial motor neuron diseaseG12.25 Progressive spinal muscle atrophyG12.29 Other motor neuron diseaseG12.8 Other spinal muscular atrophies and related syndromesG12.9 Spinal muscular atrophy, unspecifiedG14 Postpolio syndromeG35 Multiple sclerosisG70.00 Myasthenia gravis without (acute) exacerbationG70.01 Myasthenia gravis with (acute) exacerbationG71.00 Muscular dystrophy, unspecifiedG71.01 Duchenne or Becker muscular dystrophyG71.02 Facioscapulohumeral muscular dystrophyG71.031 Autosomal dominant limb girdle muscular dystrophyG71.032 Autosomal recessive limb girdle muscular dystrophy due to calpain-3 dysfunctionG71.033 Limb girdle muscular dystrophy due to dysferlin dysfunctionG71.0340 Limb girdle muscular dystrophy due to sarcoglycan dysfunction, unspecifiedG71.0341 Limb girdle muscular dystrophy due to alpha sarcoglycan dysfunctionG71.0342 Limb girdle muscular dystrophy due to beta sarcoglycan dysfunctionG71.0349 Limb girdle muscular dystrophy due to other sarcoglycan dysfunctionG71.035 Limb girdle muscular dystrophy due to anoctamin-5 dysfunctionG71.038 Other limb girdle muscular dystrophyG71.039 Limb girdle muscular dystrophy, unspecifiedG71.09 Other specified muscular dystrophiesG71.11 Myotonic muscular dystrophyG71.12 Myotonia congenitaG71.13 Myotonic chondrodystrophyG71.14 Drug induced myotoniaG71.19 Other specified myotonic disordersG71.20 Congenital myopathy, unspecifiedG71.21 Nemaline myopathyG71.220 X-linked myotubular myopathyG71.228 Other centronuclear myopathyG71.29 Other congenital myopathyG71.3 Mitochondrial myopathy, not elsewhere classifiedG71.8 Other primary disorders of musclesG72.0 Drug-induced myopathyG72.1 Alcoholic myopathyG72.2 Myopathy due to other toxic agentsG72.41 Inclusion body myositis [IBM]G72.49 Other inflammatory and immune myopathies, not elsewhere classifiedG72.89 Other specified myopathiesG72.9 Myopathy, unspecifiedG73.7 Myopathy in diseases classified elsewhereG80.0 Spastic quadriplegic cerebral palsyG82.50 Quadriplegia, unspecifiedG82.51 Quadriplegia, C1-C4 completeG82.52 Quadriplegia, C1-C4 incompleteG82.53 Quadriplegia, C5-C7 completeG82.54 Quadriplegia, C5-C7 incompleteJ98.6 Disorders of diaphragmM33.02 Juvenile dermatomyositis with myopathyM33.12 Other dermatomyositis with myopathyM33.22 Polymyositis with myopathyM33.92 Dermatopolymyositis, unspecified with myopathyM34.82 Systemic sclerosis with myopathyM35.03 Sjogren syndrome with myopathy
LCD for Cough Assist E0482

BiWaze Brochure
Patient Guide

BiWaze E0482 Rx
E0483 High Frequency Chest Wall Oscillation “Afflovest”
"High frequency chest wall oscillation" (HFCWO) refers to a chest physical therapy technique where an inflatable vest is worn, which vibrates at a high frequency to loosen and thin mucus in the airways, essentially mimicking a cough-like action to help clear secretions from the lungs; it's often used by individuals with conditions like cystic fibrosis or bronchiectasis where mucus clearance can be difficult.
Medicare requirements for bronchiectasis:
https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleId=52494
Required: CT Scan confirming diagnosis of bronchiectasis.
AND
2. Required: Daily productive cough for at least 6 continuous months.
OR
Frequent (i.e. more than 2/year) exacerbations requiring antibiotic therapy.
AND
3. Required: Documentation (chart notes) of another treatment (flutter valve,
percussion, postural drainage, breathing techniques, suctioning) tried to mobilize
secretions and clearly indicating the other technique or device has failed.
ICD-10 Code Description
J47.0Bronchiectasis with acute lower respiratory infection
J47.1Bronchiectasis with acute exacerbation
J47.9Bronchiectasis, uncomplicated
Q33.4Congenital bronchiectasis
Medicare requirements for other respiratory disorders, cystic fibrosis, neuromuscular conditions:
1. Include the covered ICD-10 diagnosis
2. Chart notes supporting the need for airway clearance for the diagnosis code
3. Details of tried, failed, or deemed inappropriate treatments (device or therapy)
BCBS of Alabama Policy:
NEW E0469 - Oscillation and Lung Expansion therapy (OLE) - Volara (acute care only), BiWave Clear (acute and home), etc
CPEP Continuous Positive Expiratory Pressure treats and helps prevent pulmonary atelectasis by combining continuous positive pressure with aerosol medication, to help expand and hold the airways open.
CHFO Continuous High Frequency Oscillation, a pneumatic form of chest therapy, delivers continuous pulses of positive pressure combined with aerosol medication to mobilize and treat retained secretions.
Nebulizer Integrated with CPEP and CHFO, medication is delivered during therapy to help loosen secretions.
https://www.hillrom.com/en/products/volara-acute-care/
https://abmrc.com/biwaze-clear-home-care/
NEW E0469 - Oscillation and Lung Expansion therapy (OLE) - Volara (acute care only), BiWave Clear (acute and home), etc
CPEP Continuous Positive Expiratory Pressure treats and helps prevent pulmonary atelectasis by combining continuous positive pressure with aerosol medication, to help expand and hold the airways open.
CHFO Continuous High Frequency Oscillation, a pneumatic form of chest therapy, delivers continuous pulses of positive pressure combined with aerosol medication to mobilize and treat retained secretions.
Nebulizer Integrated with CPEP and CHFO, medication is delivered during therapy to help loosen secretions.
https://www.hillrom.com/en/products/volara-acute-care/
https://abmrc.com/biwaze-clear-home-care/